
HISTORY AND GENERAL PRINCIPLES
Electro-acupuncture, the application of a pulsating electrical current to acupuncture needles as a means of stimulating the acupoints, was developed in China as an extension of hand manipulation of acupuncture needles around 1934. It is described, though only briefly, in most comprehensive texts of acupuncture (1-4). The procedure for electro-acupuncture is to insert the acupuncture needle as would normally be done, attain the qi reaction by hand manipulation, and then attach an electrode to the needle to provide continued stimulation. The benefits of using electrical stimulation are:
- It substitutes for prolonged hand maneuvering. This helps assure that the patient gets the amount of stimulation needed, because the practitioner may otherwise pause due to fatigue. Electro-acupuncture may also help reduce total treatment time by providing the continued stimulus. During electro-acupuncture, the practitioner can attend to other patients.
- It can produce a stronger stimulation, if desired, without causing tissue damage associated with twirling and lifting and thrusting the needle. Strong stimulation may be needed for difficult cases of neuralgia or paralysis.
- It is easier to control the frequency of the stimulus and the amount of stimulus than with hand manipulation of the needles.
The main disadvantage of electrical stimulation of acupuncture needles is the lack of direct practitioner participation in this aspect of acupuncture therapy and the associated limited opportunity for the practitioner to respond to changes that are taking place during treatment. However, for practitioners who, after inserting and initially stimulating the needles, normally leave the patient to rest undisturbed without performing prolonged needle manipulation, electro-acupuncture can provide a significant benefit: replacing the missing stimulus that is recommended by most experienced acupuncturists in China.
Although electro-acupuncture may be used as a component of nearly all acupuncture treatments that require manipulation of the needles, according to the Chinese literature, especially good results are expected from electro-acupuncture treatment of neurological diseases, including chronic pain, spasm, and paralysis. In patients with serious cardiac diseases, however, the method should be used with caution. It is generally recommended to avoid placing electrodes near the heart, as the heart can respond adversely to electrical impulses, and the path between any two electrodes should not cross the heart area, despite the low current that is used. Some have suggested avoiding placing electrodes to needles on both sides of the spinal cord (e.g., for Hua Tuo or bladder meridian points), because of the possible effect of the electrical stimulus on the nervous system. Points are generally selected in pairs for electrical pulse stimulation, with 1-3 pairs at one time, and the pairs are usually on the same side of the body.
THE USE OF ELECTRICAL STIMULATION DEVICES
The electro-acupuncture device is not intended to provide a significant current between the acupuncture needles. Rather, it delivers about 10-80 milliamps depending upon the selected setting. But, it will provide a significant voltage: 40-80 volts, which is the basis for the patient response. In the commonly-used portable battery devices, this is accomplished by boosting the voltage output of the battery, such as raising the voltage from 9 volts to 45 volts. Many of the devices have an AC adapter to avoid frequent replacement of batteries, and this involves a substantial step-down of both voltage and amperage. There is virtually no current transmitted through the body, but there is enough voltage stimulus for the patient to feel it; often this will be a pulsating sensation because of the intention of using a waveform that is perceptible.
Duration of standard treatment with electro-acupuncture is usually 10-20 minutes and rarely exceeds 30 minutes. The electrical pulsing stimulus is used in a few cases for an hour or more, especially for difficult to treat neurological disorders. During the stimulation period, the patient may become adapted to the stimulus (this will typically happen after the first minute or two), with a gradual decline in response. The electrical output should then be adjusted in frequency and/or intensity to resume the sensation. Variable frequency output of the electro-acupuncture device is sometimes utilized in an attempt to circumvent this adaptation.
Electro-acupuncture is normally administered with alternating current. Therefore, the two electrodes in any pair are equivalent, even if they are color coded to distinguish them. Some devices allow a direct current (non-alternating) setting, but the use of this has been discouraged, as mild adverse effects might occur if the pulsing of the current ceases for any reason (i.e., device defect). Further, it has been suggested, though it remains to be proven, that the adaptation to the direct current may be more rapid than to the alternating current. When it is said in electro-acupuncture literature that "the negative electrode is attached to what is considered the main point, while the positive electrode is attached to a secondary point," the statement has no relevance when using an alternating current.
The device to be used for electro-acupuncture (see Figure 1 for modern example) must have good control over its voltage output to avoid excessive electrical stimulation, namely an unexpected higher voltage pulse that causes pain or muscular contraction, and to assure that the frequency and intensity is maintained as set by the practitioner. Informal testing of devices has showed that some are erratic in their output, so older devices, and those not produced with adequate quality control measures, are to be avoided. A device commonly used in China is the G6805 or G6805-2 electric stimulator.
The device should not be turned on until after the acupuncture needles are in place and the electrodes connected. All changes in the electrical stimulus should be carried out gradually. It is normal for the patient to experience responses such as rhythmic spasm or weak twitching of the muscle (frequently visible to the practitioner), as well as the usual "deqi" reactions of acupuncture therapy: sensation of numbness, distention, and/or heaviness. The stimulus intensity, set by a voltage-adjusting knob on the device, should be in the range between the minimum amount needed for the patient to sense its effect and the minimum amount that produces an uncomfortable reaction; care should be taken to limit the muscle twitching to a mild response. Areas that are particularly sensitive to electrical stimulation are the face and regions below the elbow and knee. These areas should be treated initially with a very low intensity voltage. Patients who have not had acupuncture previously should receive standard acupuncture first to assure that they tolerate the treatment well, before moving on to electro-acupuncture, which may yield a stronger sensation.
The wave form (squared off or sharp; dense, sparse, mixed dense and sparse, or interrupted; see Figure 2 for sample outputs) can provide slightly different responses and must be tried for each patient to evaluate their suitability. Claims that one form is tonifying and another is dispersing may not be justified due to lack of adequate testing to support such differentiation of effects. A continuous wave (frequency doesn't change over time) is most similar to what acupuncturists in China attempt to administer by the manual method. The overall frequency of stimulus (either by continuous wave or pulses of dense waves) should be set similar to the frequency that would be used in manual stimulation by twirling or lifting/thrusting. Frequencies as high as 200 pulses per minute have been recommended for scalp acupuncture, with low frequencies being more commonly mentioned for body acupuncture (e.g., 50 or less). Different authors writing about electro-acupuncture present differing opinions on the ideal frequency for various desired effects. All the wave forms and frequencies are claimed to be of value in promoting circulation of qi and blood and alleviating various symptoms, particularly pain.
Although some theories have been developed regarding the mechanism of action of electro-acupuncture, there are no conclusive tests. The main function of electro-acupuncture, as evidenced by the discussions in several clinical reports in the Chinese medical literature, appears to be no more than pulsation by voltage spikes serving as stimulus replacing a rhythmic physical movement as stimulus at the site.
MEDICAL REPORTS FROM CHINA
The majority of journal articles from China on electro-acupuncture are devoted to laboratory animal studies, mainly with mice or rabbits. Those studies have limited relevance to humans because of difficulties matching points on these animals with those on humans, and the possible unique effects of electricity in small animals because of the close proximity of points, which can make the effect of the electric voltage, current, and associated electromagnetic fields more evident than would be the case in humans. It is rarely indicated by these animal studies that the effects are different from standard acupuncture manipulation, though it would be difficult to carry out prolonged manual manipulation on small animals. Thus, electro-acupuncture animal studies mainly provide a means of using an animal model to study acupuncture therapy in general.
An extensive review of the Chinese acupuncture literature shows that most clinical work with acupuncture is carried out with manual stimulus despite the ready availability of electro-acupuncture devices. In clinical trials where electro-acupuncture is used, there are few details, if any, reported about the technique, other than the duration of stimulus and the frequency of the electrical output. In one study of treatment of depression in which some explanation was given (5), the authors stated that "The intensity of stimulation was optimal when slight muscle twitching was visible, yet the patient was comfortable and the stimulus tolerable. The frequency of stimulus chosen was about 80-90 beats per minute. The duration of treatment was 1 hour each time, once a day (except Sundays) for 5 weeks, altogether 30 needlings." The authors expressed the belief, based on animal studies of electro-acupuncture, that the treatment would promote production of neurotransmitters that would alleviate the brain dysfunction. The same kind of biochemical response has been suggested as the mechanism for standard (non-electric stimulated) acupuncture.
Zheng Qiwei, an acupuncturist at the China Academy of Traditional Chinese Medicine wrote an article on point selection for electro-acupuncture (6). He first mentioned that electro-acupuncture is used the same as standard acupuncture but that electro-acupuncture therapy "has certain peculiarities and limitations because electro-acupuncture apparatus cannot be connected with all the acupoints...." Also, he mentioned that electro-acupuncture is particularly relied upon for treatment of pain, flaccidity syndromes, paralysis due to stroke, and facial paralysis of various causes. These disorders often require extensive manipulation of the needles, for which electro-acupuncture serves as a useful substitute.
As to the treatment of pain, Zheng suggests that the following points can be chosen (included, in some cases, is the "ashi" point, or point that is tender to the touch, and not necessarily a meridian point location as listed below):
- trigeminal neuralgia: zanzhu (BL-2) and yangbai (GB-14) for the first nerve branch; sibai (ST-2) with xiaguan (ST-7) or quanliao (SI-18) for the second branch; chengjiang (CV-24) and xiaguan (ST-7) for the third branch.
- sciatica: points are selected from huantiao (GB-30), zhibian (BL-54), yanglingquan (GB-34), xuanzhong (GB-39), yinmen (BL-37), and weizhong (BL-40).
- pain of greater occipital nerve: fengchi (GB-20) and an ashi point.
- migraine: fengchi (GB-20) and shuaigu (GB-8).
- periarthritis of the shoulder: select from jianyu (LI-15), jianliao (TB-14), jianzhen (SI-9), naohui (TB-13), binao (LI-14) and quchi (LI-11).
- injury of the knee joint ligaments: liangqiu (ST-34) and dubi (ST-35).
- tennis elbow: quchi (LI-11) and ashi point.
- kidney pain: jingmen (GB-25) and ashi point.
- abdominal pain: bilateral tianshu (ST-25).
- intestinal adhesion pain: local points on both ends of the operation scar.
- bone fracture: use points at the center of the fracture and at the ends of the fracture zone (e.g., for humerus fracture, jianyu (LI-15) and quchi (LI-11) represent the ends of the fracture zone; for femoral fracture, xuehai (SP-10) and biguan (ST-31) are the ends).
For flaccidity (wei) syndromes, he mentions the following points (note: when large numbers of points are offered, he recommends to select either 2 or 4 of the points to needle with electrical stimulus; the sets of points needled can vary from day to day, alternating from one set to the other and back again):
- paraplegia: select from biguan (ST-31), futu (ST-32), zusanli (ST-36), and jiexi (ST-41) as one group; a second group is zhibian (BL-54), chengfu (BL-36), yinmen (BL-37), weizhong (BL-40), chengshan (BL-57), and kunlun (BL-60).
- hemiplegia: jugu (LI-16), jianyu (LI-15), jianliao (TB-14), binao (LI-14), quchi (LI-11), waiguan (TB-5), shousanli (LI-10), and hegu (LI-4) are used for upper extremity paralysis; huantiao (GB-30), biguan (ST-31), zusanli (ST-36), yanglingquan (GB-34), sanyinjiao (SP-6), and jiexi (ST-41) for paralysis of the lower extremities.
- facial paralysis: do not use electro-acupuncture in the initial phase, as it may cause spasm. It can be used at the later stage, for example: taiyang (extra point) and zanzhu (BL-2) or sibai (ST-2) for incomplete closing of the eye; yingxiang (LI-20 and quanliao (SI-18 or xiaguan (ST-7) for difficulty sniffing; either dicang (ST-4) and jiache (ST-6) or xiaguan (ST-7 and dicang (ST-4) for difficulty in blowing out the cheeks; and heliao (LI-19) and dicang (ST-4) for deviation of the philtrum.
In addition to treatment of local points for pain or paralysis or other disorders, distal points may also be selected along the course of the meridians that flow through the area to be treated. In cases of one-sided ailments, such as arthritis in one shoulder, tennis elbow, or trigeminal neuralgia, Zheng considers it acceptable to select points on the opposite side of the body for treatment in cases where the patient may not tolerate local treatment or where local treatment might cause spasms.
Gu Yuehua, at the Nanjing College of Traditional Chinese Medicine described the use of electro-acupuncture for treatment of acute abdomen (7). This is a severe abdominal pain that can be due to several causes including renal or gallbladder colic associated with stones, acute appendicitis, dysmenorrhea (especially that due to endometriosis), and gastric spasms. Gu reported on several recommended sets of points for electroacupuncture, as follows:
- Gastric spasm: zhongwan (CV-12), juque (CV-14), and zusanli (ST-36); this point set could be modified for cold syndrome-add liangmen (ST-21)-or hot syndrome-add quchi (LI-11); for distending pain in the hypochondriac region, add taizhong (LV-3). Points were treated bilaterally where that applies.
- Billiary colic: riyue (GB-24), burong (ST-19), juque (CV-14), dannang (extra-35), and zusanli (ST-36). These points were all on the right side only.
- Renal colic: shenshu (BL-23), jingmen (GB-25), sanyinjiao (SP-6), and fujie (SP-14) all on the side affected; and yanglingquan (GB-34) bilaterally.
- Dysmenorrhea: guanyuan (CV-4) and bilateral guilai (ST-29) and sanyinjiao (SP-6); with obvious stagnation of qi and blood, add bilateral taichong (LV-3) and diji (SP-8).
He noted that most points were punctured perpendicularly, but that riyue (GB-24) and burong (ST-19) were punctured obliquely. The initial stimulus by hand was with the reducing method, with swift lifting, slow thrusting, and large amplitude rotation. After the needle sensation was felt and radiated to the affected area, electro-stimulation was added. He used a dense-disperse wave (alternating high frequency with low frequency output), with a frequency of 18 per minute (this is the frequency of dense wave outputs). The electrical stimulation was given for 30-60 minutes, with an intensity that depended on the patient's tolerance. The time required to get pain relief varied from an average of 11 minutes for "functional pain" (as, for example, with gastric spasms), to an average of 32 minutes for "organic pain" (as, for example, with renal stones). Up to 60 minutes treatment might be needed in cases where pain relief at the original site was attained, but there was still tenderness and radiating pain with pressure.
A report of using electro-acupuncture plus moxibustion for sports injury was made by Yang Jun of the Department of Acupuncture at the Anhui College of Traditional Chinese Medicine (8). Femoral adductor syndrome (pain in the pubic and medial femoral regions, exacerbated by walking or squatting) was treated with the main points yinlingquan (SP-9), qugu (CV-2), yinlian (LV-11), and an ashi point. Auxiliary points for the treatment included chengfu (BL-36), ciliao (BL-32), fengshi (GB-31), and wuli (LV-10); all of the main points and one or two auxiliary points were used for each treatment. After the needling sensation was attained, electric stimulation was applied for 15 minutes. After removing the needles, moxibustion was applied using cones on the main points for 10-15 minutes. This treatment was given once every other day, with 10 sessions one course of treatment (hence, three weeks treatment time). Yang differentiated the role of electro-acupuncture, which he said treated the subjective symptoms by promoting the flow of qi and blood and relieving pain, from that of moxibustion, which he said treated the root cause, by additionally warming the channels and removing blood stasis.
For treatment of chronic shoulder-arm pain and numbness of various causes, Liu Hongyan and Zhang Caihong claimed use of electro-acupuncture at bingfeng (SI-12) was a useful treatment (9). As auxiliary points, hegu (LI-4) would be added if the pain and numbness extended to the thumb and index fingers; zhongzhu (TB-3) was used if it extended to the ring and small fingers; and sanyinjiao (SP-6) was used when there had been a prolonged pain syndrome and muscular atrophy as a result. After getting the needle sensation, the electro-stimulation with dense wave was administered for 20 minutes once per day, with 10 days treatment constituting a course of therapy. Although improvements could be noted after just one or four treatments for many patients, some had to undergo one to two course of therapy or more to get adequate relief.
In a report of acupuncture therapy for post-herpetic neuralgia (10), two groups of points were selected: the Hua Tuo jiaji that corresponded to the painful area to be treated by electric stimulation, and limb points selected on the basis of syndrome differentiation to be treated by manual stimulation. Thus, patients with diagnosis of qi stagnation and blood stasis were manually treated at zhigou (TB-6), yanglingquan (GB-34), xuehai (SP-10), and sanyinjiao (SP-6); patients with deficiency of yin were treated at laogong (PC-8), taixi (KI-3), and fuliu (KI-7); while patents with stagnation of damp-heat were treated at quchi (LI-11), yinlingquan (SP-9), and sanyinjiao (SP-6). For the Hua Tuo points, needling was first performed unilaterally on the painful side, using 3-5 needles with about 1 cun space between needles, using slight oblique insertion towards the spine. After arrival of qi attained with lifting and thrusting, the needles were connected to the electric stimulator device with continuous wave, with 40-50 minutes stimulus. The limb points were then needled and stimulated every few minutes over the same time period. Ten daily treatments constituted a course of therapy, which could be repeated after a three day interval.
In a study of electro-acupuncture therapy given to cancer patients after chemotherapy (11), needles were applied to zusanli (ST-36), sanyinjiao (SP-6), zhongwan (CV-12), and neiguan (PC-6). The method of therapy was described as follows:
The patient was asked to take the supine position. After needling sensation was attained, the needles were connected to the G-6805 electro-acupuncture apparatus with disperse-tense wave at an intensity tolerable to the patient. The treatment was given for 30 minutes once daily, five daily sessions constituting one course of treatment, with an interval of 2 days between courses.
Four courses of therapy (four weeks, with 5 days therapy followed by 2 days off each week) were administered to evaluate the effects, which were claimed to be beneficial and involved an average 5-10% increase in subsets of T-cells and a 15% increase in natural killer cell activity (however, there was not control group for comparison). It was also claimed to improve appetite and sleep, relieve tumor pain, and alleviate the gastro-intestinal reactions to chemotherapy.
SUMMARY
Electro-acupuncture is a convenient stimulation technique to be utilized with the same acupuncture points and the same number of treatments as with manual acupuncture. For busy practitioners and those who do not normally provide prolonged manual needle stimulation, even when it is normally called for according to Chinese literature, electro-acupuncture may improve the clinical situation. In cases where intensive, high frequency, and prolonged treatments might be deemed essential, as with certain stubborn neurological disorders, electro-acupuncture may be the only means to provide effective daily treatments. Practitioners should consult literature accompanying the device they purchase regarding contraindications for electro-acupuncture and recommendations for using different pulse forms and frequencies, but should also be aware that there may be very limited basis for some of the statements that are made.
REFERENCES
- Chinese Academy of Traditional Chinese Medicine, An Outline of Chinese Acupuncture, 1975 Foreign Languages Press, Beijing.
- O'Connor J and Bensky D (translators), Acupuncture: A Comprehensive Text, 198 Eastland Press, Seattle, WA.
- Zhang Enquin (editor in chief), Chinese Acupuncture and Moxibustion, 1990 Publishing House of Shanghai College of Traditional Chinese Medicine, Shanghai.
- Dang Yi (chief editor, English), Acupuncture and Moxibustion, 1999 Academy Press, Beijing.
- Luo Hechun, Jia Yunkui, and Zhanli, Electro-acupuncture vs. amitriptyline in the treatment of depressive states, Journal of Traditional Chinese Medicine 1985; 5(1): 3-8.
- Zheng Qiwei, Experience in the point selection for electro-acupuncture, Journal of Traditional Chinese Medicine 1998; 18(4): 277-281.
- Gu Yuehua, Treatment of acute abdomen by electro-acupuncture, Journal of Traditional Chinese Medicine 1992; 12(2): 110-113.
- Yang Jun, 32 cases of femoral adductor syndrome treated by electro-acupuncture and moxibustion, Journal of Traditional Chinese Medicine 1998; 18(4): 263-264.
- Liu Hongyan and Zhang Caihong, 60 cases of shoulder-arm syndrome treated by electro-acupuncture at bingfeng (SI-12), Journal of Traditional Chinese Medicine 1998; 18(4): 256-258.
- Wu Jianhui and Guo Zhili, 23 cases of postherpetic neuralgia treated by acupuncture, Journal of Traditional Chinese Medicine 2000; 20(1): 36-37.
- Ye Fang, Chen Shaozong, and Liu Weiming, Effects of electro-acupuncture on immune function after chemotherapy in 28 cases, Journal of Traditional Chinese Medicine 2002; 22(1): 21-23.
NOTE: In this article, the term electro-acupuncture refers solely to stimulation of acupuncture needles by a pulsed electric voltage for the purpose of providing a stimulus similar to that obtained by manual needle manipulation. This is the definition and application of electro-acupuncture as described in literature from China. Unfortunately, the term electro-acupuncture has been used by Vohl and others who apply it to describe diagnostic methods that are not permitted in the acupuncturist scope of practice, and for which there is no viable evidence that either the diagnostic or the associated treatment methods accomplish what is claimed. In addition, the term electro-acupuncture has been used to describe the TENS device and its use in treatment with microcurrent applied (usually without acupuncture needles) to a segment of the skin or muscles, which is not addressed in this article. Many of the electro-acupuncture devices made in the U.S. are designed for use in both electro-acupuncture and TENS treatment.
August 2002

Figure 1: An electro-acupuncture stimulator.
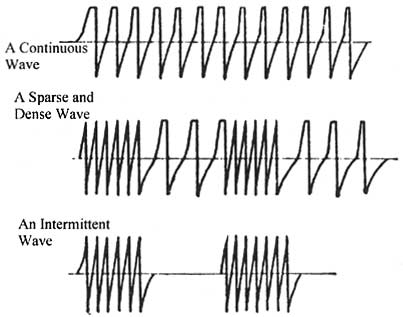
Figure 2: Samples of wave forms produced by electro-acupuncture devices.
0 komentar:
Posting Komentar